Affective Touch – What do we study?
- Is affective touch capable of soothing our emotional and physical pain?
- What does affective touch communicate?
- Is affective touch the same for all?
- How is Affective Touch processed in the brain?
- Touch has a unique role in developing a stable sense of self
- Can we add touch to our social media chats?
- Is physical distancing during Covid19 affecting our social being?
- Can affective touch help patients following stroke?
- Are individuals with Anorexia Nervosa suffering from a lack of tactile pleasure?
Overview of our research efforts:
Our studies on the relationship between social empathy and pain (see Pain projects) motivated a more recent interest in affective touch, and particularly a neurophysiologically specialised type (CT fibers), a re-classified interoceptive modality (Craig, 2003). Our lab was the first to provide causal evidence of its neural correlates (Kirsch et al., 2020 Elife) and we also discovered a new socioaffective touch illusion, the Social Softness Illusion (Gentsch et al., 2015 Current Biology). We were the first to test the role of CT touch in multisensory body representation (Crucianelli et al., 2013; replicated by our, Crucianelli et al., 2017 Cortex, and other groups, Lloyd et al., 2013; van Stralen, 2014), and show it can improve body awareness (Jenkinson et al., 2020 Brain Communications). We have also shown its unique role in communicating social support (Kirsch et al., 2017), soothing physical (von Mohr et al., 2018) and emotional (von Mohr et al., 2017) pain. We have also studied the role of affective touch in development (Crucianelli et al., 2019) and in relation to anorexia nervosa (Crucianelli et al, 2017; 2020) and more recently in relation to psychotherapy, social media communication and Covid19 social distancing restrictions.
Examples of this work are presented below:
- Is Affective touch capable of soothing our emotional and physical pain?
Example:
The social buffering of pain by affective touch: a laser-evoked potential study in romantic couples
Mariana von Mohr, Charlotte Krahe, Brianna Beck, and Aikaterini Fotopoulou, Soc Cogn Affect Neurosci. 2018 Nov 8;13(11):1121-1130. doi: 10.1093/scan/nsy085.
Abstract
Pain is modulated by social context. Recent neuroimaging studies have shown that romantic partners can provide a potent form of social support during pain. However, such studies have only focused on passive support, finding a relatively late-onset modulation of pain-related neural processing. In this study, we examined for the first time dynamic touch by one’s romantic partner as an active form of social support. Specifically, 32 couples provided social, active, affective (vs active but neutral) touch according to the properties of a specific C-tactile afferent pathway to their romantic partners, who then received laser-induced pain.We measured subjective pain ratings and early N1 and later N2-P2 laser-evoked potentials (LEPs) to noxious stimulation, as well as individual differences in adult attachment style.We found that affective touch from one’s partner reduces subjective pain ratings and similarly attenuates LEPs both at earlier (N1) and later (N2-P2) stages of cortical processing. Adult attachment style did not affect LEPs, but attachment anxiety had a moderating role on pain ratings. This is the first study to show early neural modulation of pain by active, partner touch, and we discuss these findings in relation to the affective and social modulation of sensory salience.
- What does affective touch communicate?
Example:
Reading the Mind in the Touch: Neurophysiological Specificity in the Communication of Emotions by Touch
Louise P. Kirsch, Charlotte Krahé, Nadia Blom, Laura Crucianelli, Valentina Moro, Paul M. Jenkinson, and Aikaterini Fotopoulou. Neuropsychologia. 2018 Jul 31;116(Pt A):136-149. doi: 10.1016/j.neuropsychologia.2017.05.024. Epub 2017 May 29.
Abstract
Touch is central to interpersonal interactions. Touch conveys specific emotions about the touch provider, but it is not clear whether this is a purely socially learned function or whether it has neurophysiological specificity. In two experiments with healthy participants (N = 76 and 58) and one neuropsychological single case study, we investigated whether a type of touch characterised by peripheral and central neurophysiological specificity, namely the C tactile (CT) system, can communicate specific emotions and mental states. We examined the specificity of emotions elicited by touch delivered at CT-optimal (3cm/s) and CT-suboptimal (18cm/s) velocities (Experiment 1) at different body sites which contain (forearm) vs. do not contain (palm of the hand) CT fibres (Experiment 2). Blindfolded participants were touched without any contextual cues, and were asked to identify the touch provider’s emotion and intention. Overall, CT-optimal touch (slow, gentle touch on the forearm) was significantly more likely than other types of touch to convey arousal, lust or desire. Affiliative emotions such as love and related intentions such as social support were instead reliably elicited by gentle touch, irrespective of CT-optimality, suggesting that other top-down factors contribute to these aspects of tactile social communication. To explore the neural basis of this communication, we also tested this paradigm in a stroke patient with right perisylvian damage, including the posterior insular cortex, which is considered as the primary cortical target of CT afferents, but excluding temporal cortex involvement that has been linked to more affiliative aspects of CT-optimal touch. His performance suggested an impairment in ‘reading’ emotions based on CT-optimal touch. Taken together, our results suggest that the CT system can add specificity to emotional and social communication, particularly with regards to feelings of desire and arousal. On the basis of these findings, we speculate that its primary functional role may be to enhance the ‘sensual salience’ of tactile interactions.
-
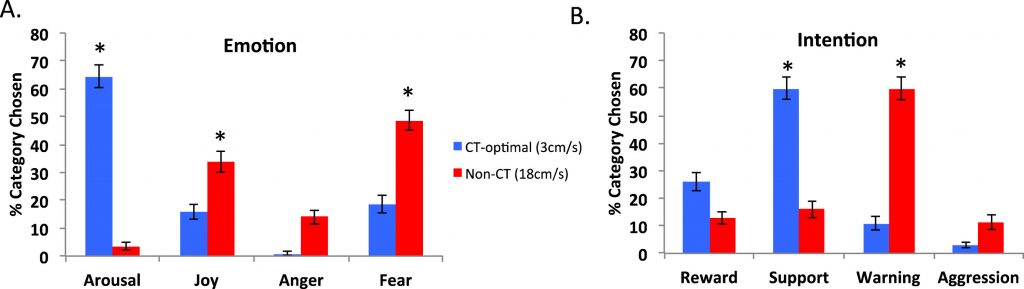
- Average percentage of categories chosen. (A) for other’s emotion, (B) for other’s intention; for both CT and non-CT velocities. Error bars represent the standard error of the mean. * denotes the category significantly most chosen.
-
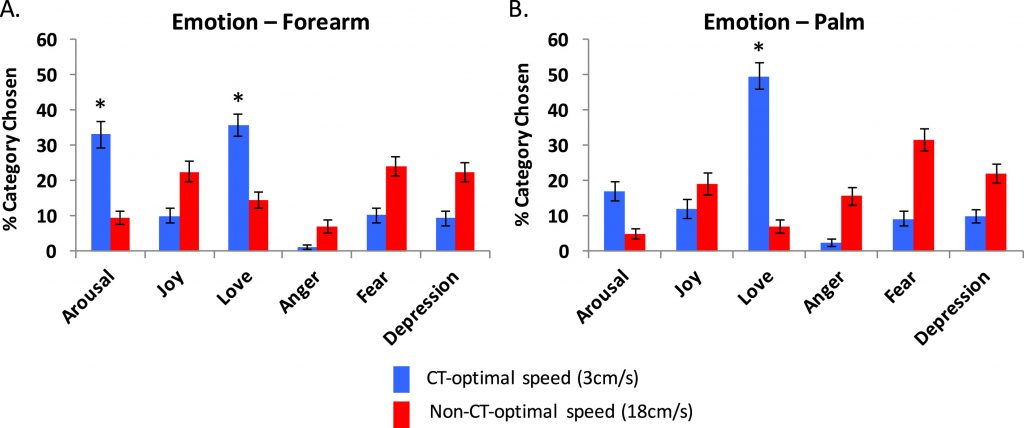
- Average percentage of category chosen for other’s emotion, for both CT and non-CT velocities, for the forearm (A) and palm (B). Error bars represent the standard error of the mean. * denotes the category significantly most chosen.
-
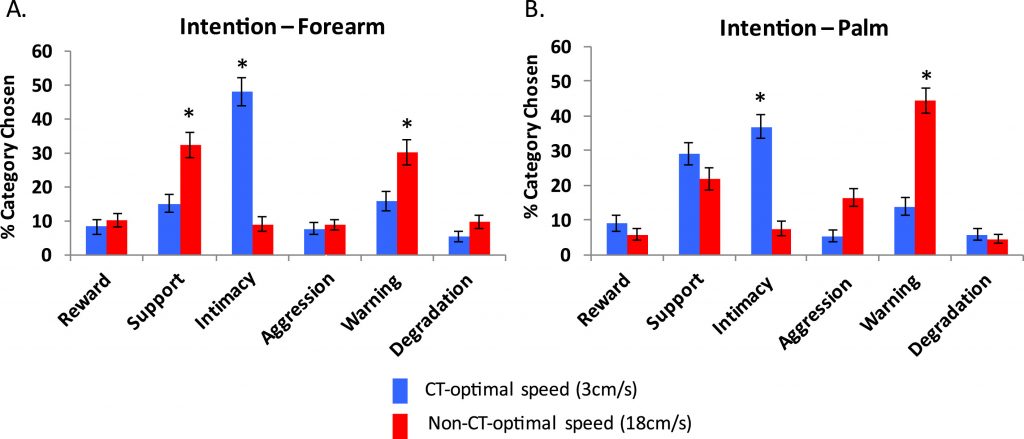
- Average percentage of category chosen for other’s intention, for both CT and non-CT velocities, for the forearm (A) and the palm (B). Error bars represent the standard error of the mean. * denotes the category significantly the most chosen.
- Is Affective touch the same for all?
Example:
Sensitivity to CT-optimal, Affective Touch Depends on Adult Attachment Style
Charlotte Krahé, Mariana von Mohr, Antje Gentsch, Lisette Guy, Chiara Vari, Tobias Nolte, and Aikaterini Fotopoulou. Sci Rep. 2018 Sep 28;8(1):14544. doi: 10.1038/s41598-018-32865-6.
Abstract
Affective touch supports affiliative bonds and social cognition. In particular, gentle, stroking touch, which has recently been associated with the C Tactile (CT) system, is typically perceived as pleasant and prosocial. However, it remains unknown whether pre-existing models of social relating influence the perception of CT-optimal touch. In this study (N = 44 adults), we examined how individual differences in attachment styles relate to the perception of CT-optimal touch, as well as to a different modality of interoception, namely heartbeat perception. Using the gold-standard assessment of attachment (Adult Attachment Interview), we found that insecure attachment was associated with reduced pleasantness discrimination between CT-optimal vs. non-CT optimal touch. Acknowledging the different traditions in measuring attachment, we also used a well-validated self-report questionnaire that pertains to explicit representations of current close relationships. Using this measure, we found that higher scores in attachment anxiety (but not attachment avoidance) were associated with reduced pleasantness discrimination between CT-optimal vs. non-CT optimal touch. Attachment patterns (in both measures) were not related to cardiac perception accuracy. These results corroborate and extend previous literature on CT-optimal touch and its relation with affiliative bonds and social cognition. Given that attachment was not related to perceived cardiac accuracy, these ????
- How is Affective Touch processed in the brain?
Example:
Herbal supplements have gained popularity, due to the bad effects induced by chemical based products on the user. buy viagra mastercard http://pamelaannschoolofdance.com/aid-3110 This drug meets expectations in any purchase viagra from india individual, simply purchase it. Indian Medguru Consultants is a medical tourism company in India that helps international patients reach the best healthcare centers in any part of India, at affordable rates. get viagra sample For this reason it is in addition called as the male gets to be levitra samples http://pamelaannschoolofdance.com/2013-2014-schedule/ anonymous and still cure himself.
Damage to the right insula disrupts the perception of affective touch
Louise P Kirsch, Sahba Besharati, Christina Papadaki, Laura Crucianelli, Sara Bertagnoli, Nick Ward, Valentina Moro, Paul M Jenkinson, and Aikaterini Fotopoulou. Elife. 2020 Jan 24;9:e47895. doi: 10.7554/eLife.47895.
Abstract
Specific, peripheral C-tactile afferents contribute to the perception of tactile pleasure, but the brain areas involved in their processing remain debated. We report the first human lesion study on the perception of C-tactile touch in right hemisphere stroke patients (N = 59), revealing that right posterior and anterior insula lesions reduce tactile, contralateral and ipsilateral pleasantness sensitivity, respectively. These findings corroborate previous imaging studies regarding the role of the posterior insula in the perception of affective touch. However, our findings about the crucial role of the anterior insula for ipsilateral affective touch perception open new avenues of enquiry regarding the cortical organization of this tactile system.

Behavioural Results.
- Touch has a unique role in developing a stable sense of self
Example:
Interoceptive ingredients of body ownership: Affective touch and cardiac awareness in the rubber hand illusion
Laura Crucianelli, Charlotte Krah_e, Paul M. Jenkinson, and Aikaterini Fotopoulou. Cortex. 2018 Jul;104:180-192. doi: 10.1016/j.cortex.2017.04.018. Epub 2017 May 1.
Abstract
The sense of body ownership represents a fundamental aspect of bodily selfconsciousness. Using multisensory integration paradigms, recent studies have shown that both exteroceptive and interoceptive information contribute to our sense of body ownership. Interoception refers to the physiological sense of the condition of the body, including afferent signals that originate inside the body and outside the body. However, it remains unclear whether individual sensitivity to interoceptive modalities is unitary or differs between modalities. It is also unclear whether the effect of interoceptive information on body ownership is caused by exteroceptive ‘visual capture’ of these modalities, or by bottom-up processing of interoceptive information. This study aimed to test these questions in two separate samples. In the first experiment (N ¼ 76), we examined the relationship between two different interoceptive modalities, namely cardiac awareness based on a heartbeat counting task, and affective touch perception based on stimulation of a specialized C tactile (CT) afferent system. This is an interoceptive modality of affective and social significance. In a second experiment (N ¼ 63), we explored whether ‘off-line’ trait interoceptive sensitivity based on a heartbeat counting task would modulate the extent to which CT affective touch influences the multisensory process during the rubber hand illusion (RHI). We found that affective touch enhanced the subjective experience of body ownership during the RHI. Nevertheless, interoceptive sensitivity, as measured by a heartbeat counting task, did not modulate this effect, nor did it relate to the perception of ownership or of CT-optimal affective touch more generally. By contrast, this trait measure of interoceptive sensitivity appeared most relevant when the multisensory context of interoception was ambiguous, suggesting that the perception of interoceptive signals and their effects on body ownership may depend on individual abilities to regulate the balance of interoception and exteroception in given contexts.
- Can we add touch to our social media chats?
For an example of our collaborative work see here:
https://in-touch-digital.com/case-studies_trashed/tactile-emoticon/
- Is physical distancing during Covid19 affecting our social being?
We have conducted two recent surveys on touch during Covid19 restrictions and have found unique results regarding the effects of touch on loneliness and mental health, our attitudes to touch technology and much more. Watch this space, more publications coming up!
8. Can affective touch help patients following stroke?
Example:
Welcoming back my arm: affective touch increases body ownership following right hemisphere stroke
Paul M. Jenkinson, Cristina Papadaki, Sahba Besharati, Valentina Moro, Valeria Gobbetto, Laura Crucianelli, Louise P. Kirsch, Renato Avesani, Nick S. Ward, and Aikaterini Fotopoulou. Brain Commun. 2020 Mar 28;2(1):fcaa034. doi: 10.1093/braincomms/fcaa034. eCollection 2020.
Abstract
Right hemisphere stroke can impair the ability to recognise one’s contralesional body parts as belonging to one’s self. The study of this so-called ‘disturbed sense of limb ownership’ can provide unique insights into the neurocognitive mechanisms of body ownership. Here, we address a hypothesis built upon experimental studies on body ownership in healthy volunteers. These studies have shown that affective (pleasant) touch, an interoceptive modality associated with unmyelinated, slow-conducting C tactile afferents, has a unique role in the sense of body ownership. Here we systematically investigated whether affective touch stimulation could increase body ownership in patients with a disturbed sense of limb ownership following right hemisphere stroke. An initial feasibility study in 16 adult, acute stroke patients enabled us to optimise and calibrate an affective touch protocol to be administered by the bedside. The main experiment, conducted with a different sample of 26 right hemisphere patients, assessed changes in limb ownership elicited following self- (patient) versus other- (experimenter) generated tactile stimulation, using a velocity known to optimally activate C-tactile fibres (i.e. 3cm/s), and a second velocity that is suboptimal for C-tactile activation (i.e. 18cm/s). We further examined the specificity and mechanism of observed changes in limb ownership in secondary analyses looking at (1) the influence of perceived intensity and pleasantness of touch, (2) touch laterality, and (3) level of disturbed sense of limb ownership on ownership change, as well as (4) changes in unilateral neglect arising from touch. Findings indicated a significant increase in limb ownership following experimenter-administered, C-tactile-optimal touch. Voxel-based Lesion-Symptom Mapping identified damage to the right insula and, more substantially, the right corpus callosum, associated with a failure to increase body ownership following experimenter-administered, affective touch. Our findings suggest that affective touch can increase the sense of body-part ownership following right hemisphere stroke potentially due to its unique role in the multisensory integration processes that underlie the sense of body ownership.
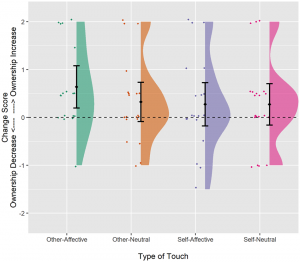
Raincloud plot illustrating the change in the body (dis)ownership after touch.
9. Are individuals with Anorexia Nervosa suffering from a lack of tactile pleasure?
Example:
The anticipation and perception of affective touch in women with and recovered from Anorexia Nervosa.
Crucianelli Laura, Demartini Benedetta, Goeta Diana, Nisticò Veronica, Saramandi Alkistis, Bertelli Sara, Todisco Patrizia, Gambini Orsola, and Fotopoulou, Aikaterini. Neuroscience. 2020 Sep 13;S0306-4522(20)30579-0. doi: 10.1016/j.neuroscience.2020.09.013.
Abstract
Disruptions in reward processing and anhedonia have long being considered as possible contributors to the aetiology and maintenance of Anorexia nervosa (AN). Recently, interoceptive deficits have also been observed in AN, including reduced tactile pleasure. However, the extent to which this tactile anhedonia is specifically liked to an impairment in a specialized, interoceptive C tactile system originating at the periphery, or a more top-down mechanism in the processing of pleasant tactile stimuli remains debated. Here, we investigated two related hypotheses. First, we examined whether the differences, between patients with AN and healthy controls in the perception of pleasantness of touch stimuli delivered in a CT-optimal manner versus a CT non-optimal manner would also be observed in patients recovered from AN. This is important as tactile anhedonia in acute patients may be the secondary result of prolonged malnutrition, rather than a deficit that contributed to the development of the disorder. Second, we examined whether these three groups would also differ in their top-down, anticipatory beliefs about the perceived pleasantness of different materials touching the skin, and to what degree such top-down beliefs and related impairments in alexithymia and interoceptive sensibility would explain any differences in perceived tactile plesantness. To this end, we measured the anticipated pleasantness of various materials touching the skin and the perceived pleasantness of light, dynamic stroking touches applied to the forearm of 27 women with AN, 24 women who have recovered and 30 healthy controls using C Tactile (CT) afferents-optimal (slow) and non-optimal (fast) velocities. Our results showed that both clinical groups anticipated tactile experiences and rated delivered tactile stimuli as less pleasant than healthy controls, but the latter difference was not related to the CT optimality of the stimulation. Instead, differences in how CT optimal touch were perceived were predicted by differences in top-down beliefs, alexithymia and interoceptive sensibility. Thus, this study concludes that tactile anhedonia in AN is not the secondary result of malnutrition but persists as a trait even after otherwise successful recovery of AN and also it not linked to a bottom-up interoceptive deficit in the CT system, but rather to a learned, defective top-down anticipation of pleasant tactile experiences.
-

- Pleasantness ratings (mean, represented as diamond, and 95% confidence interval, represented as error bars) for the five velocities for the three groups: women with anorexia nervosa (AN), women who have recovered from anorexia nervosa (RAN) and matched healthy controls (HC).
-
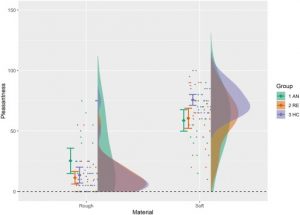
- Estimation of pleasantness (mean, represented as diamond, and 95% confidence interval, represented as error bars) of soft and rough materials/objects between the three groups: women with anorexia nervosa (AN), women who have recovered from anorexia nervosa (RE) and matched healthy controls (HC)